
SMART
Intestinal Stent Implantation: An Endoluminal Minimally Invasive Interventional Solution for Malignant Bowel Obstruction
Malignant bowel obstruction (MBO) is a common and severe complication in patients with advanced abdominal malignancy. Traditional emergency open surgery is associated with substantial trauma, high complication rates, and often requires enterostomy. As a well-established endoluminal interventional technique, intestinal stent implantation serves as a pivotal minimally invasive solution for palliative treatment and bridge-to-surgery management of malignant bowel obstruction.
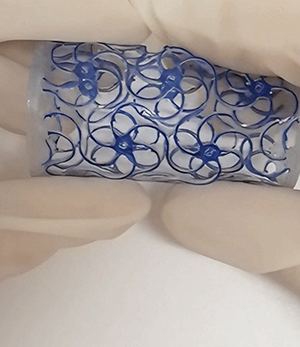
Intestinal stents are typically woven from nitinol alloy with superelasticity and shape memory effect. Their core mechanism lies in pre-compression and loading into a delivery system, which is then delivered to the intestinal stenotic lesion through the natural orifice under imaging guidance (e.g., fluoroscopy) or direct endoscopic visualization. Upon deployment, the stent spontaneously expands to the preset diameter at body temperature, achieving mechanical dilation of the obstructed segment, restoring intestinal lumen patency, and enabling rapid relief of obstruction.
The standard clinical procedure adheres to minimally invasive principles: performed by an interventional endoscopist or interventional radiologist, the procedure is conducted under sedation or anesthesia. A working channel is established via colonoscope or duodenoscope; the stent is precisely positioned under guidewire guidance and then deployed. Postoperatively, imaging examinations are conducted to assess stent position and expansion status.
II. Clinical Positioning: Clear Indications and Treatment Objectives
The clinical application of this technique centers on two definitive treatment objectives, with indication selection requiring rigorous evaluation by a multidisciplinary team (MDT):
Palliative therapy: For permanent bowel obstruction induced by unresectable advanced or metastatic tumors, stent implantation aims to restore intestinal patency, alleviate symptoms such as vomiting and abdominal distension, enable patients to resume oral intake, and avoid long-term nasogastric decompression or surgical enterostomy. It effectively improves the quality of life (QoL) of terminal-stage patients, serving as an active palliative supportive treatment.
Technical Advantages
Minimally invasive nature: Avoids open surgery and related trauma
Immediate patency: Obstruction symptoms usually resolve rapidly within 24–72 hours
Therapeutic optimization window: Enables neoadjuvant therapy or general condition improvement in bridge-to-surgery scenarios
Quality of life improvement: Demonstrates significant efficacy in palliative treatment
Technical vs. clinical success: Technical success refers to accurate stent deployment and expansion, while clinical success means sustained symptom relief. Both are affected by lesion characteristics (length, angle, location), operator experience and patient-related factors.
Anatomical constraints: Current technology is more suitable for colonic, rectal and duodenal obstruction. Stent application for jejunoileal obstruction remains challenging due to bowel tortuosity and difficult fixation, which is one of the key directions for ongoing research and technical refinement.
IV. Cutting-edge Advances and Future Directions
Current research and development focus on optimizing stent performance to overcome existing limitations:
Material and structural innovation: Developing new covered stents (partial or fully covered) to reduce tumor ingrowth; exploring biodegradable stent materials to eliminate permanent implantation.
Functionalized stents: Investigating drug-eluting stents (e.g., loaded with chemotherapeutic or targeted drugs) to achieve local anti-tumor therapy.
Delivery system improvement: Developing more flexible and precisely controllable delivery devices for implantation in complex anatomical sites.
Combined treatment strategies: Exploring comprehensive regimens integrating stent implantation with local radiotherapy, photodynamic therapy, etc.
Intestinal stent implantation is a well-established endoluminal interventional technique with irreplaceable value in the management system of malignant bowel obstruction. Its successful application relies on precise patient selection, standardized technical operation and an MDT-based diagnostic and treatment model. Future technological development will further enhance its efficacy and safety, and expand clinical application boundaries through interdisciplinary integration of materials science, engineering and oncology.
The content of this article is based on current clinical practice and academic consensus, intended for professional information exchange only. Specific clinical decisions must be made by medical professionals based on individual patient conditions.